Female Pattern Hair Loss (Androgenetic Alopecia) — A Physician's Guide
Part of: Women's Hair Loss — A Physician's Clinical Knowledge Center
By Dr. Susan Lin, M.D. — Board-Certified OB/GYN & Anti-Aging Medicine Physician. Reviewed: May 2026.
The short answer
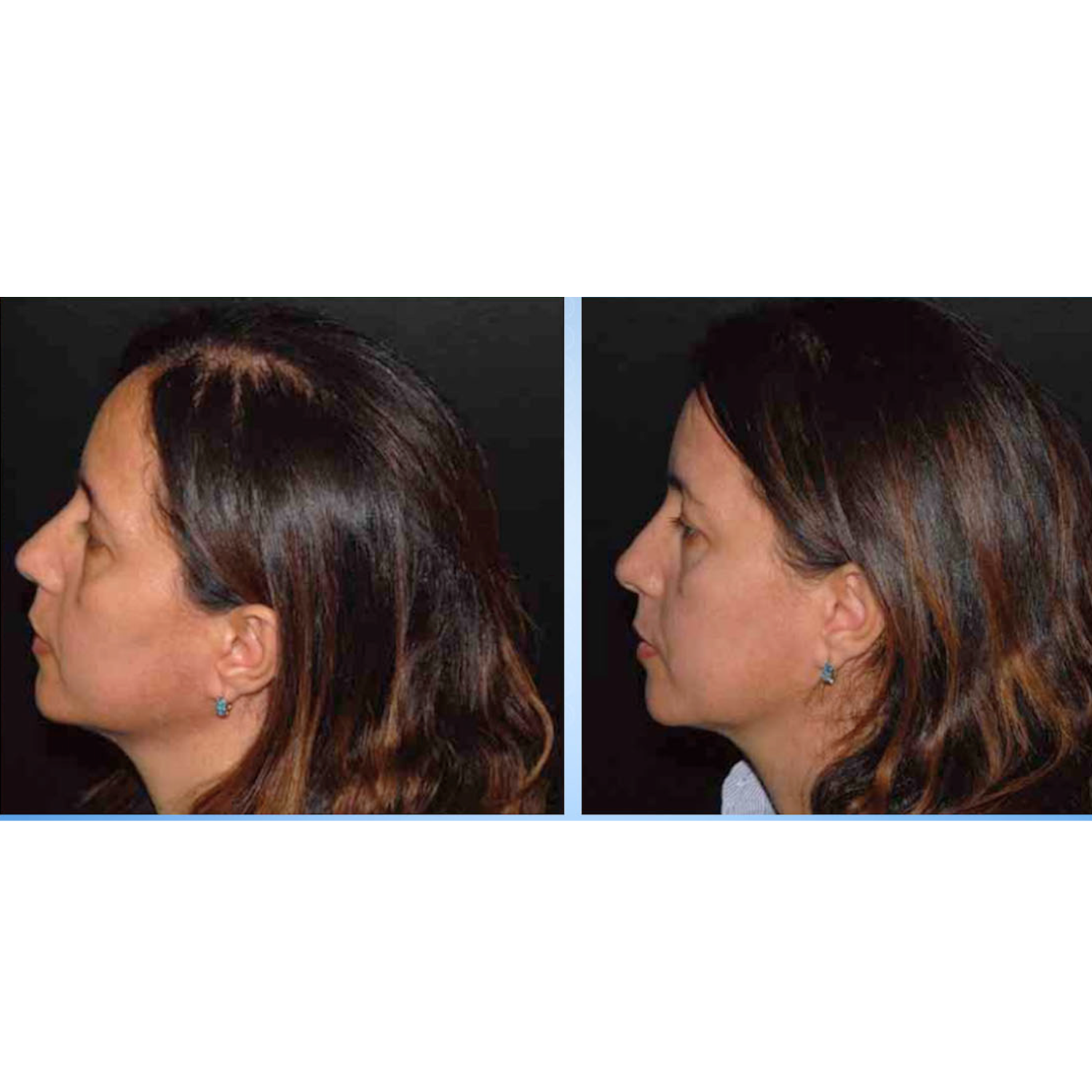
Female pattern hair loss (FPHL) — clinically called androgenetic alopecia in women — affects approximately 30-40% of women by age 60, with some women noticing the first signs as early as their 20s or 30s. Unlike postpartum shedding (acute) or menopause thinning (estrogen-driven), FPHL is a chronic, progressive, genetically determined condition driven by an inherited sensitivity of scalp follicles to DHT. The classic pattern: a widening of the part line ("Christmas tree" pattern) and diffuse thinning across the top of the scalp, with the frontal hairline characteristically preserved. FPHL cannot be cured, but it is highly responsive to sustained, drug-free intervention that modulates the DHT pathway and supports follicle wellness.
What FPHL looks like — the pattern
| Feature | Female pattern (FPHL) | Male pattern (MPB) |
|---|---|---|
| Frontal hairline | Preserved | Recedes (M-shape) |
| Crown | Diffuse thinning | Crown baldness common |
| Part line | Progressive widening (Christmas tree) | N/A |
| Complete baldness | Rare | Common |
The Ludwig Scale grades FPHL severity:
- Ludwig I — early widening of part line; mild thinning
- Ludwig II — moderate diffuse thinning; part clearly wider; scalp visible
- Ludwig III — advanced thinning; significant visible scalp; very sparse coverage on top
Why FPHL happens — the biology
- Genetic predisposition — polygenic inheritance. If your mother, grandmother, or sisters have thinning, your risk is elevated.
- DHT sensitivity at the scalp — Genetically susceptible follicles express more 5-alpha reductase (testosterone→DHT) and more androgen receptors. DHT binding causes follicle miniaturization over time.
- Diminished anagen phase — Growth phase shortens. Hair never reaches its full potential length or thickness.
FPHL is not caused by elevated androgens in most women. Total testosterone levels are usually normal. The issue is follicular sensitivity to normal androgen levels — a genetic trait, not an endocrine disease.
When to suspect FPHL vs other women's hair loss
FPHL has distinguishing features: gradual onset (months to years), diffuse thinning across the top of the scalp, preserved frontal hairline, family history of thinning, Christmas tree pattern at the part, no scalp symptoms (no pain, scaling, or redness), no bald patches.
When FPHL needs a deeper workup
- Onset is unusually early (teens or early 20s) — may suggest PCOS or other endocrine cause
- Accompanied by hirsutism, severe acne, or menstrual irregularity — suggests androgen excess
- Rapid progression — uncommon for FPHL
- Scalp symptoms — suggests scarring alopecia or scalp disease
Workup labs: CBC, ferritin, TSH, free T4, vitamin D, B12, total and free testosterone, DHEA-S, prolactin, (and glucose tolerance / lipids if PCOS suspected).
The drug-free recovery framework for FPHL
Because the mechanism is DHT sensitivity, the framework emphasizes DHT modulation alongside follicle support.
1. Internal DHT modulation
MD Nutri Hair delivers Lilac extract titrated for verbascoside (natural DHT pathway modulator), marine collagen, biotin, flaxseed lignans, vitamin E. Drug-free, hormone-free, no contraindications for childbearing women.
2. Topical scalp environment with saw palmetto and peptides
MD Follicle Energizer combines saw palmetto (natural 5-alpha-reductase inhibitor) with Biotinoyl Tripeptide-1. MD Follicle Activator with Acetyl Tetrapeptide-3 and Red Clover Extract supports follicle anchoring.
3. Scalp environment — gentle, non-stripping
MD Revitalizing Treatment Shampoo and Conditioner with patented StimuCap® peptide technology. Sulfate-free, silicone-free, safe for color-treated hair.
4. Complete system — the MD Hair Restoration Kit
The MD Hair Restoration Kit bundles scalp serum + topical activator + oral supplement into a coordinated 3-step protocol — the most comprehensive drug-free approach for FPHL.
5. Nutritional repletion
Baseline labs and repletion of ferritin (>70), vitamin D (30-60), B12, protein (1.0-1.2 g/kg).
What about pharmaceutical options?
Topical minoxidil — FDA-approved for women, modestly effective, requires lifelong use. Side effects: scalp irritation, unwanted facial hair growth, initial increased shedding. Safety in pregnancy/breastfeeding not established. Oral finasteride / dutasteride — Off-label, contraindicated for women of childbearing potential (teratogenic). Spironolactone — Off-label, requires monitoring. Hair transplantation — Effective but expensive; requires sufficient donor density.
For most women with mild-to-moderate FPHL — especially those of childbearing potential, pregnant, breastfeeding, or who prefer non-pharmaceutical approaches — the drug-free framework is the appropriate first-line.
What NOT to do
- Do not over-diagnose yourself with FPHL if you have a recent clear acute trigger (likely telogen effluvium)
- Do not start finasteride without specific physician supervision — contraindicated for women of childbearing potential
- Do not expect quick results — the follicle cycle takes 3-6 months to respond
- Do not pull hair into tight ponytails, buns, or braids (traction alopecia)
- Do not use harsh sulfate growth shampoos
- Do not over-color or chemically over-process thinning hair
Frequently asked questions
Q: At what age does FPHL start?
A: As early as late teens or 20s in susceptible women; most women first notice in their 30s-50s. Often accelerates at menopause.
Q: Is FPHL reversible?
A: Not curable, but highly manageable. Most women see meaningful stabilization or improvement within 3-6 months with drug-free intervention.
Q: How is FPHL different from telogen effluvium?
A: Telogen effluvium is acute and self-limited; FPHL is gradual, chronic, and progressive.
Q: Can MD Nutri Hair help FPHL?
A: Yes. Lilac extract verbascoside directly addresses the DHT pathway. Drug-free, hormone-free.
Q: Will I need MD Hair products forever?
A: For FPHL, sustained use is appropriate — genetic predisposition doesn't change. Discontinuing typically results in gradual return of thinning.
Q: Does FPHL cause complete baldness?
A: Rarely. Severe FPHL results in significantly thinned hair with visible scalp, but typically with some coverage remaining.
Bottom line
FPHL is common, genetic, and chronic — but highly treatable with a thoughtful drug-free framework. Three principles: start early (preserves more existing follicle density), use a multi-pathway system (DHT modulation + scalp wellness + nutrition), commit to consistency (3-6 months minimum, sustained long-term).
Related reading
Featured products
Cited literature
- Lin, S. F. (Fall 2012). Medical Female Hair Loss. The National Hair & Skin Journal, 16(63), 10–11. — Dr. Lin's published clinical framework for female hair loss including FPHL.
- Lin, S. F. (April 2017). Novel Drug-Free Hair Loss Treatment. Euro Cosmetics. — Verbascoside action on 5-alpha-reductase isoforms 1 and 2; the mechanistic foundation for drug-free DHT modulation in FPHL.
- Lin, S. F. (2013). Stem Cells: The Recent Innovation in Hair Regeneration. The Link — The Voice of the American Hair Loss Council, Issue 7, p. 5.
- Olsen EA. Female pattern hair loss. J Am Acad Dermatol. 2001;45(3 Suppl):S70-S80.
- Prager N et al. Botanical 5-alpha-reductase inhibitors in androgenetic alopecia. J Altern Complement Med. 2002;8(2):143-52.
Educational only; not a substitute for individualized medical advice.