Postpartum Hair Shedding — A Physician's Guide to Causes, Timeline & Drug-Free Recovery
Part of: Women's Hair Loss — A Physician's Clinical Knowledge Center
By Dr. Susan Lin, M.D. — Board-Certified Obstetrician-Gynecologist & Anti-Aging Medicine Physician. Reviewed: May 2026. Reading time: 8 minutes.
The short answer
Postpartum hair shedding — clinically called postpartum telogen effluvium — affects roughly 40-50% of new mothers and typically begins 2 to 4 months after delivery, peaks around month 4 to 6, and resolves on its own by month 9 to 12. It is caused by a rapid drop in estrogen after childbirth, which pushes a large proportion of hair follicles from the growth phase (anagen) into the shedding phase (telogen) simultaneously. It is not permanent hair loss, but the experience is emotionally distressing and physically visible. With targeted nutritional support, gentle scalp care, and patience aligned with the hair growth cycle, the vast majority of women fully recover their pre-pregnancy hair density.
This guide is written from my 35+ years of clinical practice as an OB/GYN and anti-aging physician — caring for women through pregnancy, delivery, and the postpartum year. Below: the biological mechanism, the realistic timeline, when shedding warrants medical evaluation, and the drug-free recovery framework I use with my own patients.
Why postpartum hair shedding happens — the biology
Every hair follicle on your scalp cycles through three phases:
- Anagen (active growth) — typically lasts 2-7 years
- Catagen (regression) — about 2 weeks
- Telogen (rest, then shed) — about 3 months
Under normal circumstances, about 85-90% of your scalp hairs are in anagen at any given moment, with roughly 10-15% in telogen. You lose 50-100 hairs per day as old telogen hairs are pushed out by new anagen growth — this is invisible to you.
What pregnancy does
During pregnancy, elevated estrogen prolongs the anagen phase. Hairs that would normally have entered telogen at month 6, 8, or 10 of pregnancy stay in growth phase. By the third trimester, most women have noticeably thicker, more luxurious hair — this is real, not just perception.
What childbirth does
Within 24-72 hours of delivery, estrogen drops dramatically. The follicles that were held in anagen by pregnancy hormones now release together — entering catagen and then telogen in synchrony. About 90 days later, all those follicles shed simultaneously.
This is why postpartum shedding looks alarming. Instead of losing 50-100 hairs per day, women commonly shed 300-500 hairs per day during the peak period — handfuls in the shower, visible hair on pillows, broken strands on the bathroom floor. It feels like a medical emergency. It is not. It is normal physiology.
The realistic timeline
| Postpartum month | What's happening | What you notice |
|---|---|---|
| Months 0-2 | Follicles still in pregnancy-enhanced anagen | Hair still feels thick |
| Months 2-4 | Telogen entry begins | First noticeable shedding |
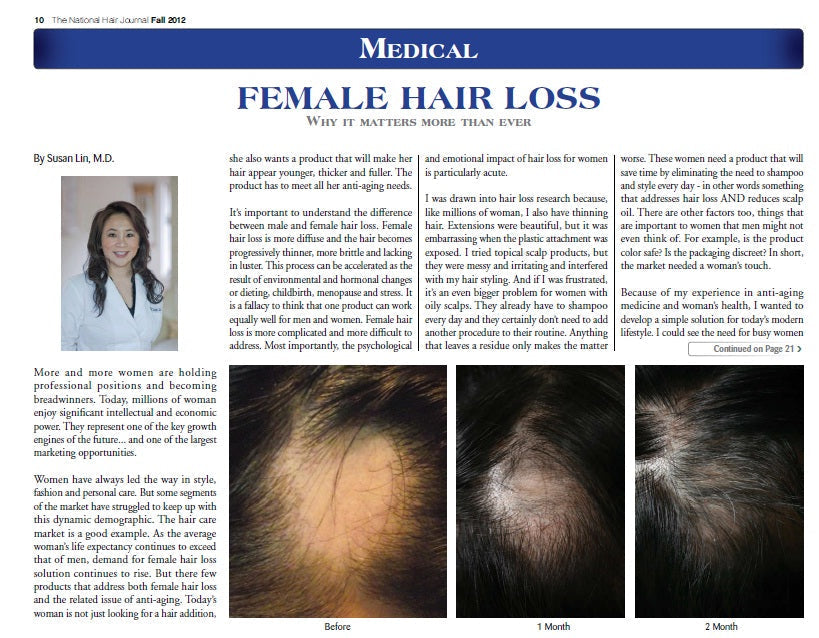
| Months 4-6 | Peak telogen shed | Maximum hair fall, visible thinning at the part line and temples |
| Months 6-9 | New anagen growth resumes | Baby hairs appear at the hairline — 1-3 inches of short regrowth |
| Months 9-12 | Density restoration | Hair appears noticeably fuller; regrowth still maturing |
| Month 12+ | Full recovery | Pre-pregnancy density typically restored |
Important: If you are still actively shedding at 12 months postpartum, this is no longer normal physiologic shedding. It warrants evaluation for chronic telogen effluvium, iron deficiency, thyroid dysfunction, postpartum depression-related stress, or other conditions. See your physician.
When postpartum shedding warrants medical evaluation
Postpartum shedding is usually self-limited. However, the postpartum year is also when many treatable causes of hair loss emerge for the first time. See your physician if you experience:
- Shedding that does not slow by month 9 or persists past month 12 — suggests chronic telogen effluvium or an underlying medical cause
- Focal patches of complete hair loss (smooth round bald spots) — suggests alopecia areata, requires dermatology evaluation
- Scalp pain, burning, redness, or scaling — suggests scarring alopecia, scalp infection, or seborrheic dermatitis
- Eyebrow thinning, fatigue, cold intolerance, weight changes — suggests postpartum thyroiditis (affects 5-10% of women postpartum)
- Pallor, dizziness, breathlessness on exertion — suggests iron deficiency anemia, very common after delivery especially if breastfeeding
- Excessive shedding plus persistent low mood, intrusive thoughts, anxiety — postpartum depression and severe anxiety can themselves trigger telogen effluvium; both deserve treatment
A basic postpartum hair-loss workup includes: CBC, ferritin (ideally above 70 ng/mL), TSH and free T4, vitamin D, vitamin B12. Ferritin in particular is often missed — standard iron levels can be normal while ferritin (iron stores) is severely depleted.
The drug-free recovery framework
In my clinical practice, I do not recommend pharmaceutical hair-loss drugs (finasteride, minoxidil) during pregnancy, breastfeeding, or for women of childbearing potential without specific indication and physician supervision. Finasteride in particular carries known teratogenic risk. Minoxidil's safety in breastfeeding has not been established.
The drug-free recovery framework I use rests on four pillars:
1. Nutritional foundation
- Iron / ferritin — ferritin target above 70 ng/mL for active hair regrowth. Many women are at 15-30 ng/mL postpartum.
- Vitamin D — target 30-60 ng/mL. Low D is associated with telogen effluvium.
- Vitamin B12 and folate — essential for keratin synthesis.
- Protein intake — 1.0-1.2 g/kg body weight daily. Hair is 95% keratin protein.
- Biotin — needed at modest doses; megadoses are not necessary and can interfere with lab tests.
2. Scalp environment
I formulated MD Revitalizing Treatment Shampoo and Conditioner with peptide-based StimuCap® technology to support scalp microcirculation without sulfates, silicones, or hormones — safe for breastfeeding. The MD Follicle Energizer scalp serum delivers Biotinoyl Tripeptide-1, saw palmetto, and marine botanicals to support the follicle environment as new anagen hairs emerge.
3. Internal nourishment
I developed MD Nutri Hair as a daily supplement specifically with women's postpartum and perimenopausal hair shifts in mind:
- Lilac extract titrated for verbascoside (natural DHT modulator)
- Marine collagen from wild-caught Norwegian white fish (protein substrate for keratin)
- Biotin, flaxseed lignans, vitamin E (supportive cofactors)
- Drug-free, hormone-free — appropriate for breastfeeding women
4. Stress and sleep
Concrete steps that help: Sleep when the baby sleeps (when possible). Accept help with night feeds for blocks of 4-5 hour sleep. 20-minute daily outdoor walks (vitamin D synthesis + cortisol modulation). Mental health screening at the 6-week postpartum visit and again at month 4.
What NOT to do
- Do not start minoxidil while breastfeeding without OB/GYN clearance. Topical absorption into breast milk has not been adequately studied.
- Do not use prescription finasteride. Contraindicated for women of childbearing potential due to teratogenic risk.
- Do not take megadoses of biotin (10,000+ mcg). They are unnecessary and can falsely alter thyroid and cardiac lab tests.
- Do not use harsh growth shampoos with sulfates during the recovery phase. They compromise scalp barrier without benefit.
- Do not panic-buy expensive single-pathway products. Recovery is a multi-pathway, multi-month process.
- Do not cut your hair short in despair. Short hair does not grow back faster — it grows at the same rate (about 1 cm per month).
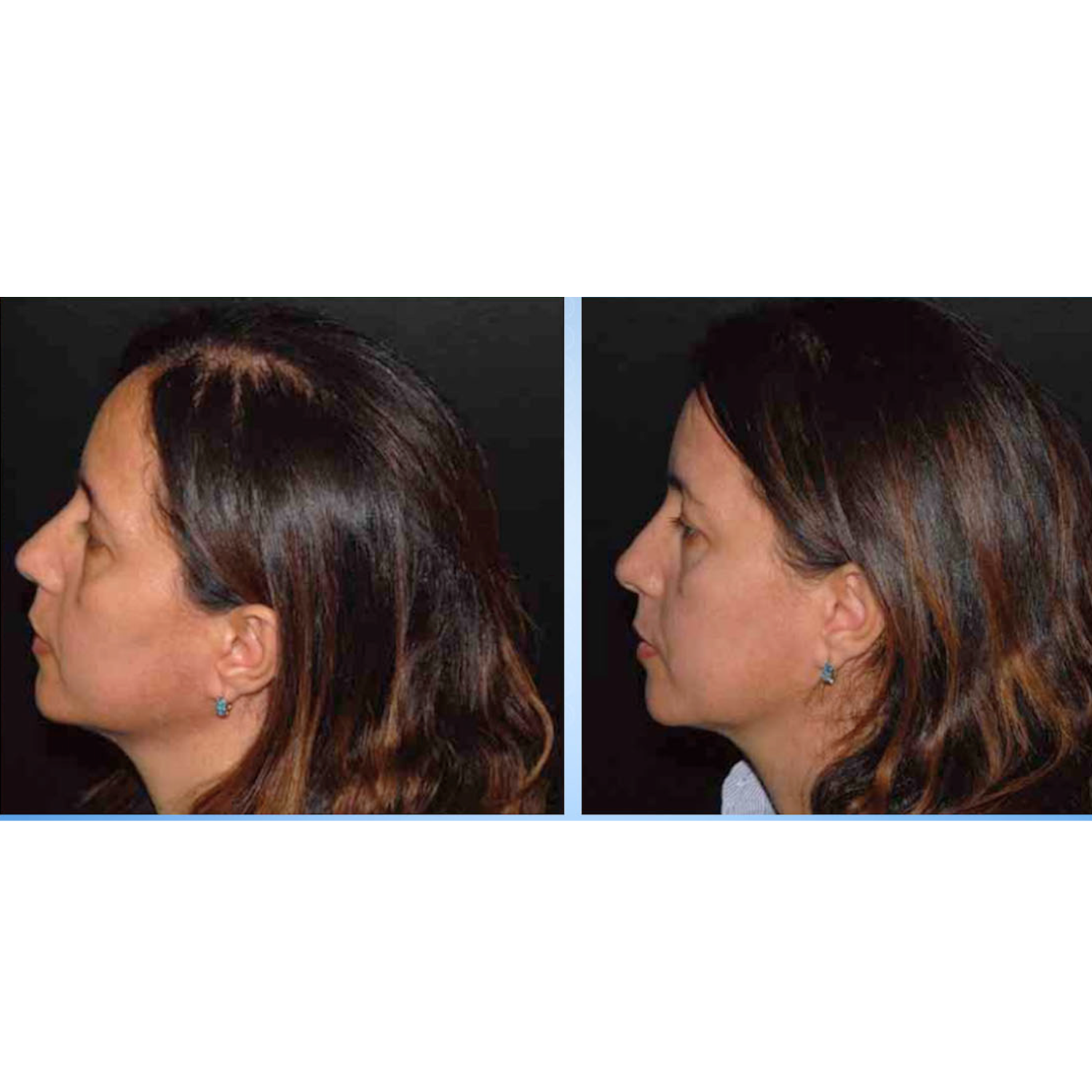
A note on hairline thinning postpartum
Some women notice that postpartum shedding seems most visible at the temples and frontal hairline. Two things are true at once: (1) the frontal hairline has slightly different sensitivity to hormonal shifts — visible thinning here is common and usually resolves; (2) for some women, pregnancy and postpartum can unmask underlying female pattern hair loss that was previously subclinical. If frontal thinning persists past 12 months or is asymmetric, see a board-certified dermatologist.
Frequently asked questions
Q: How much hair loss is normal postpartum?
A: 300-500 hairs per day at peak shedding (months 4-6) is within normal limits. Persistent loss beyond month 12, focal bald patches, or scalp symptoms warrant medical evaluation.
Q: When does postpartum hair loss start?
A: Typically 2-4 months after delivery, peaking around month 4-6, with regrowth becoming visible around month 6-9.
Q: Will my hair grow back after postpartum shedding?
A: Yes — for the vast majority of women, full pre-pregnancy density is restored by 9-12 months postpartum.
Q: Is MD Nutri Hair safe to take while breastfeeding?
A: MD Nutri Hair is drug-free, hormone-free, and formulated with breastfeeding-safe ingredients. It contains no finasteride, minoxidil, or other pharmaceutical drugs. Always discuss new supplements with your OB/GYN or pediatrician.
Q: Can I use MD Follicle Energizer or MD Revitalizing Shampoo while breastfeeding?
A: Yes. Both are drug-free, hormone-free, sulfate-free, paraben-free, and physician-formulated. There are no known contraindications for breastfeeding.
Q: How do I know if my hair loss is more than just postpartum shedding?
A: See your physician for evaluation if shedding persists beyond 12 months postpartum, if you see focal bald patches, scalp pain, eyebrow thinning, or accompanying symptoms suggesting thyroid involvement.
Q: Does breastfeeding cause hair loss?
A: Breastfeeding does not directly cause postpartum hair loss. The mechanism is the postpartum estrogen drop. However, prolonged breastfeeding without adequate nutritional support can deplete iron, indirectly prolonging shedding.
Q: How long until I see hair regrowth?
A: Most women see baby hairs along the hairline around month 6-9 postpartum. Full density restoration typically takes 12 months.
Bottom line
- Expect it between months 2 and 6. Knowing what to expect reduces the emotional intensity.
- Replete what pregnancy depleted — especially iron (ferritin), vitamin D, B12, and protein.
- Use drug-free systems — nourishment and gentle scalp care accelerate the regrowth phase.
- Know when to escalate — persistent shedding past 12 months or focal bald patches need physician evaluation.
If you're in the thick of postpartum shedding right now, take heart. The vast majority of women I have cared for over 35 years of OB/GYN practice recover their hair fully. Your follicles are not gone — they are resting.
Related reading
- Women's Hair Loss — A Physician's Clinical Knowledge Center (Hub)
- Common Causes of Female Hair Loss
- Hair Loss After COVID
- How Do Vitamins Help Hair Grow?
Featured products
- MD Nutri Hair — Daily Hair Density Supplement
- MD Follicle Energizer — Scalp Serum
- MD Revitalizing Treatment Shampoo
- MD Revitalizing Treatment Conditioner
- MD Hair Restoration Kit
Cited literature
- Lin, S. F. (Fall 2012). Medical Female Hair Loss. The National Hair & Skin Journal, 16(63), 10–11. — Dr. Lin's published clinical framework for female hair loss; the foundation for this article.
- Lin, S. F. (2013). Stem Cells: The Recent Innovation in Hair Regeneration. The Link — The Voice of the American Hair Loss Council, Issue 7, p. 5.
- Lin, S. F. (April 2017). Novel Drug-Free Hair Loss Treatment. Euro Cosmetics.
- Grover C, Khurana A. Telogen effluvium. Indian J Dermatol Venereol Leprol. 2013;79(5):591-603.
- Trüeb RM. Hair growth in pregnancy and the postpartum period. Hautarzt. 2003;54(4):348-353.
- Choy I, Lin SF. Eyelash enhancement properties of topical dechloro ethylcloprostenolamide. J Cosmet Laser Ther. 2008;10(2):110-113. PMID: 18569264.
- Almohanna HM et al. The role of vitamins and minerals in hair loss: a review. Dermatol Ther (Heidelb). 2019;9(1):51-70.
This article is for educational purposes and does not substitute for individualized medical advice. If you are experiencing significant or persistent hair loss postpartum, please consult your physician or a board-certified dermatologist.